Civic Imagination and the Creative Rites We Need – A conversation with Mortal Made
Photograph: Chloe Osborne and Steven Aron Williams
Mortal Made is a project created by artists Steven Aron Williams and Chloe Osborne, alongside a community of death practitioners based in east Kent. Together, they’re building creative and communal ways to engage with death, dying, and grief.
This is a conversation about what happens when death stops being something that happens to us, and starts being something we know how to hold.
Steven: When I began to travel and encounter how other cultures deal with their dead, something profoundly shifted in me. The burning ghats in Nepal. The vibrant, town-like graveyards of Mexico, where people celebrate and grieve their dead not just at funerals but woven into the fabric of everyday life, in ways that are open, honest and unapologetically colourful. Death held by communities rather than handed over to them once it was already packaged and processed. I kept coming back to the same thought: what do we lose when we lose that? Can it be reclaimed?
Chloe:What we lose, I think, is the permission. And the practice.
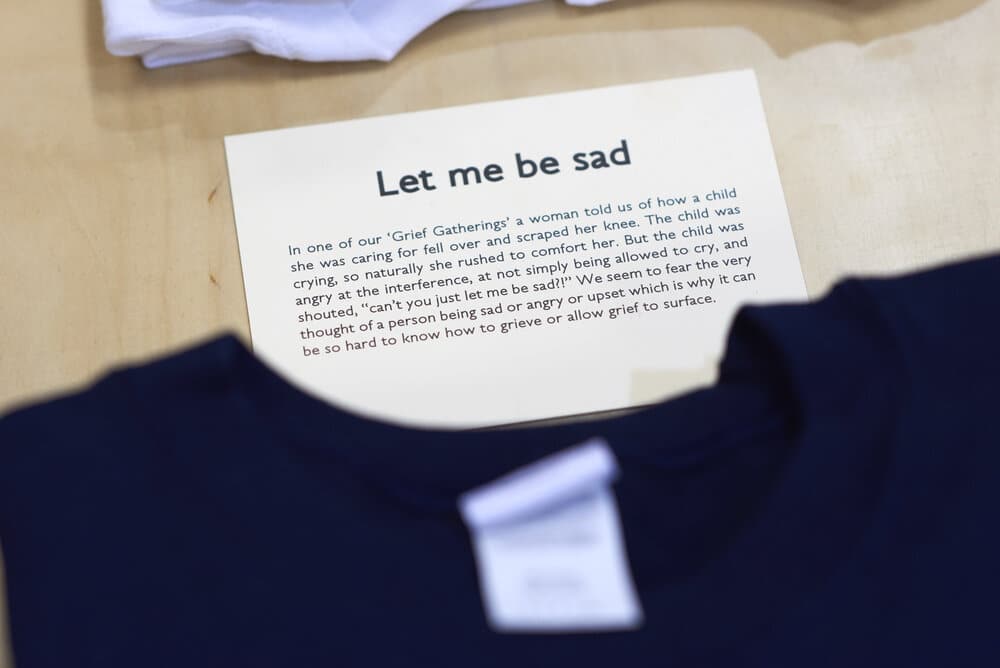
In 2020, when death got very close, very fast, for a lot of people, what I kept noticing was not sadness, exactly. It was disorientation. A kind of homesickness with nowhere to go. People did not have the language, the permission, the room. One person told me: “Grief is like being in a room by yourself, without the words to describe it or a way in or out. You can sense there are other rooms. You can feel the bigness of the house. But you can’t find the door.”
I will never forget that. It said everything about what is missing.
COFFINS Sq
SKULLS & SOULS Sq
Steven: The door exists, though. It’s just not always verbal, and it is not always arrived at through the mind. I grew up in a family where death was something that happened to adults, elsewhere, and by the time I finally encountered it directly I found myself thinking: why has nobody prepared us for this?
It was travel that began to show me what preparation could look like. Not grief as a problem to be solved, or a process to be managed, but death as something that genuinely belongs to everyone. Something you could practise. Something a community could hold together.
Chloe:That is where our creative practices come in. Steven and I both understand, from years of making, that making is a form of knowing and not simply an illustration of it. When you put your hands into clay, or sit inside the weight of a shroud. When you weave dead organic matter into a wreath for an ancestor you never met or sewing with inherited materials you are not expressing something you already understood.
You are arriving somewhere you could not have reached any other way. The material thinks with you, it can hold what words refuse to carry.
Grief lives in the body before it lives in the mind, sitting in the chest, the throat, the hands, and moments of genuine contact rarely happen through speech alone. They happen when the hands are occupied, when the body is moving, when the eye is caught by something unexpected. Sideways, through the senses, through the peripheral vision of the self. You cannot always talk your way to the door. Sometimes you have to make your way there, stumbling.
Steven: We also needed to understand the practicalities. We sat down with Toby from Simple Kent Funerals, a bottle of wine, and a whole bag of curiosities, beginning with “your person is dead” and working outwards from there through the steps and permutations, the practicalities and the possibilities, the things you are told and the many more things you are not. Three hours later we had the foundations of a Death Architecture guide, a practical map through all the choices nobody tells you exist. Apparently you can be buried in your own garden, which the neighbours might have thoughts about, but still.
Informed choice, it turns out, is an act of care.
Send Off Social Club
Chloe: That guide matters because communities that understand death make better deaths, better funerals, and better lives. But the practical and the poetic need each other, and that is why, alongside it, we built the Send Off Social Club: an experiment in what grief space looks like when it is led by the senses rather than the agenda. Opening late, offering mezcal, playing music you can move your body to. No requirement to name what you are carrying.
One person came because a friend had died in Melbourne and they had not been able to get there for the funeral. They left an offering on the community altar and buried a letter they had written. “It was beautiful and deep and healing,” they told us afterwards. “A goodbye I wouldn’t have been able to make.” They did not need a ceremony with the right words. They needed a container, permission, somewhere to put it. That is what we are trying to build. Not the correct ritual. Just the space where you can find your own.
Steven:What stays with me is how the ridiculousness comes out once people feel safe enough to let it. People laughed. People cried, often at the same time, about the same thing, and that permission to be both at once is everything. We are not built to be tidy about death and we should stop pretending otherwise.
Mortal Made came from personal curiosity and a penchant for mixing things up, but it was never designed just for us. It is for everybody, and we are looking for co-authors to join us and help shape what comes next. It does not take much.
Create the space. Offer the experience. Let people contemplate the inevitable.
Steven Aron Williams is a visual artist whose curiosity with death stems from what he sees as a cultural paralysis that afflicts the society he grew up in. Death and grief are swept under the carpet, stoicism prevails. Everything is just dealt with efficiently, the colourful craziness of life discarded. There is such a massive disconnect between the living and the dead.
His traveling has opened his eyes to the attitudes, rituals and traditions of other cultures that feel more honest and human; perhaps too honest in some instances, but he believes there is so much we can learn and take solace in.
It has also led him to contemplate his own inevitable exit. The funerals he has attended over the years (he avoids them if possible) each had a prescribed monotony that didn’t seem to really reflect the people lost. It’s such a shame and made the occasions far more traumatic than they already were.
If our exits were really contemplated, planned and shared whilst we’re still full of life, perhaps they would be more life-affirming experiences for those left behind?
Chloe Osborne has been holding arts-led spaces to explore grief and death since 2020, when for many it felt that death got so much closer. It sat differently, crouching on handrails and drifting in the air, infecting thoughts and ways of being. It was no longer an ostracised relative in a far-flung land but a close family member, sharing a bathroom.
Chloe is becoming a serial eulogist and doesn’t like it. There aren’t enough words.
What if we, as makers, doers, thinkers, sleepers and eaters, we found ways to hold ourselves and each other in grief?
What if we found and shared ways to fit the rage and grief, of genocide far away and arms made next door, inside our bodies? What if we could do this and still keep moving?
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.
8th October 2024
What does it mean to be death positive?
Anna Wilde, a PhD student based at the University of Birmingham, shares what it means to be death positive, and how talking about and preparing for death can enrich our lives, reminding us to be grateful for each day we have.
If you have come across the term ‘death positive’, perhaps on social media, you might wonder what on earth it means. After all, we know that we’re going to die and so is everyone that we care about – what is there to be positive about? And who came up with the idea, anyway?
Caitlin Doughty, the founder of the Death Positive Movement (DPM), attributes the start of the movement to asking on Twitter (now X) in 2013: “Why are there a zillion websites and references to being sex positive and nothing for being death positive?” She explained that by “death positive”, she means: “I am fascinated by death, the history of death, how cultures around the world handle death, my own relationship to mortality, and I refuse to be ashamed of that interest”.
The tweet attracted suggestions that a new movement should be formed, and Doughty, who was running her own mortuary services in Los Angeles at the time, became the founder of the Order of the Good Death, which she started with the collaboration of several other women. Doughty also set up the hugely popular@AskAMortician YouTube channel, which now has over 2.1 million subscribers; the collection spans 11 years and numbers 270 videos. She also has a large following on Instagramand other social media channels, delivers talks at death-related events worldwide and has authored three books. Through these methods, the concept of the DPM has spread and is now active in the US, Canada, the UK, Australia and New Zealand, and growing within Europe.
However, death positivity isn’t about rejoicing when someone dies, or looking forward with glee to our own final moments. It’s much more about viewing death as a natural part of life and accepting the fact that, no matter what we do to avoid it, death is inevitable for us all. People who call themselves death positive will vary in their beliefs and behaviours, but most will talk easily and naturally about death, and encourage those around them to do the same. They will suggest that everyone should have paperwork in place and share it with their family, so that when they die, all the required items such as wills, funeral wishes and financial information is readily at hand. Some death positive practitioners, such as people who work within end-of-life care or death doulas, encourage a death plan, sometimes called a ‘living will’ or ‘advance directive’ to be made, which detail your wishes on resuscitation and refusal of treatment.
But as well as these practical issues, at the heart of the DPM is the desire for everyone to have access to a ‘good death’.
Defining what constitutes a good death is difficult as it’s a very personal thing – what does it mean to die well? A hundred years ago, most people died at home, but nowadays in the UK, only about 30% of deaths occur outside of a hospital, hospice or care home, although interestingly these numbers are rising.
For my research, I interviewed people who identified as death positive on this subject, and most agreed that feeling some element of choice and control over their manner and place of death was important to them; for example, choosing not to be sedated, if possible. Of course, death, rather like birth, does not always stick to the script we give it, but it is still useful to think through our preferences. Circumstances can deprive us of choices, whether those circumstances arise due to poverty, isolation or other factors, and the Order of the Good Death advocates for people’s wishes to be honoured, regardless of their race, gender or sexual orientation.
Within the UK, adherents of the DPM are quietly working to help make dying a natural part of people’s lives. When I tell people I study death, they are either disgusted or intrigued – and nearly everyone will say: “Of course, we don’t talk about death”. I usually ask them to consider whether that oft-repeated phrase is actually still true. Across the country (and indeed, the world) Death Cafés are held regularly, where people come to explore their feelings on death, dying, grief and bereavement. Whether it’s fear of dying, the loss of a pet, the death of a beloved partner, or just plain interest, many people find great relief in discussing these things – and of course, there’s always plenty of tea and cake. There are also Death Positive Libraries, who can loan books on death such as With the End in Mind by Dr Kathryn Mannix, or Nine Rules to Conquer Death by Kevin Toolis (and many more). Various podcasts on death abound, including the award-winning Griefcast, with Radio 4presenter Cariad Lloyd, and Where There’s a Will, There’s a Wake with actor Kathy Burke. Then there’s TED talks, online festivals such as Lifting the Lid International Festival of Death and Dying, organisations such as the Good Grief Trust… all in all, too many different initiatives to mention.
Meanwhile, independent funeral directors such as Poppy’s Funeralsare committed to helping their customers achieve the funeral wishes of their loved ones. They encourage a personalised, rather than a packaged, approach and will assist you in carrying out after-death care on your relative if you would like to, by washing and dressing them. This individual approach is also seen in the funeral celebrants who will design and host a funeral alongside you, and in the many natural burial grounds that favour an eco-friendly method of body disposal, often involving cardboard or wicker coffins or woven woollen shrouds.
To end on a personal note, the reasons I began studying death were connected to my mother’s illness of being in a catatonic state with dementia for over ten years. This followed a serious road accident where I was permanently disabled. There was a lot of loss and grief surrounding both these events, and my mother’s eventual death brought some relief as I could finally remember her how she used to be, rather than how her illness had affected her. I became interested in death and its many different aspects, which led to my Masters and then PhD studies. I consider myself to be death positive, although I still fear dying, especially as I get older and closer to it! I’ve met some fascinating people through my studies, all of whom have given me different perspectives on death, which is truly multi-dimensional. From cultural perspectives to religion, body disposal to death in art, literature and the media, my work at Caring for God’s Acre and with CEDAR Education(Community Education in Death Awareness & Resources), turning to death has been very life-enhancing for me. None of us are guaranteed our tomorrows and I find talking about death and preparing for it also reminds me to be grateful for every day we have left on this beautiful earth.
Anna Wilde
Anna Wilde is researching the Death Positive Movement for her PhD at the University of Birmingham. She holds an MA in Death, Religion and Culture and works for Caring for God’s Acre, a charity that supports the environmental and built heritage of burial grounds across the UK. Anna is also a Director of CEDAR Education, which is a non-profit company working in the field of death education.
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.
24th January 2023
“Talking about dying doesn’t make it happen” – A conversation with the Waiting Room Revolution
In November 2021, Pilgrims Hospices took part in a virtual event with Canada-based podcast the Waiting Room Revolution. Dr. Andrew Thorns, Consultant in Palliative Care and former Medical Director, and Justine Robinson, Therapies and Wellbeing Manager, spoke with Dr. Hsien Seow and Dr. Samantha Winemaker about death, dying and end-of-life care in the UK and Canada.
An audio recording and a full transcript of the event are available below.
Please note:This virtual event took place in November 2021, and the information included was accurate at the time of recording.
Welcome and introductions
Dr. Hsien Seow: Welcome back to the Waiting Room Revolution. We are excited to be collaborating with the UK’s Pilgrims Hospices and have friends from across the pond on the show today. Pilgrims Hospices has been providing palliative and end-of-life care for over 38 years to the people of east Kent, which is about an hour or two east of London. It’s one of the largest hospice charities in the UK.
Today, we are thrilled to have on the show:
Dr. Andrew Thorns, who is the Medical Director for Pilgrims Hospices since 2015, and has been a palliative care consultant for over 20 years in east Kent.
Justine Robinson, who is the Therapies and Wellbeing Manager. She has been an occupational therapist for 23 years, joining Pilgrims Hospices in 2011.
Welcome both to the show today.
Andrew and Justine, maybe you could tell us a little bit about your roles and what you love about your jobs?
Dr. Andrew Thorns: Thank you, Hsien. Thank you so much for the invitation; I felt honoured to follow in the footsteps of some very distinguished people on your podcasts, which I think are excellent.
I work across Pilgrims Hospices, which is a charitable organisation that provides in-patient specialist palliative care beds and community work. I’m also a consultant at the local hospitals; we have three hospitals in the area, so I provide input into there as well, alongside five other consultant colleagues.
My need to try and save life all the time – I began to realise that wasn’t just the way to go forward. It’s much better to try and enable people to die comfortably, peacefully, at peace with themselves.
Dr. Andrew Thorns
As you go on through medicine, you realise that not everyone is going to survive. Unfortunately, we all are going to die at some point, and if you can make that last bit of people’s lives that little bit better, that little bit easier, then there’s a huge satisfaction in that. My need to try and save life all the time – I began to realise that wasn’t just the way to go forward. It’s much better to try and enable people to die comfortably, peacefully, at peace with themselves. When we achieve that, I think that’s a huge success, and I’m really pleased.
I particularly like my job when I can see people in all the different environments they find themselves in. It’s just so lovely to see people where they need to be, where they should be, managing their symptoms, their issues, supporting their families in their homes when we can. But equally, having access to our beds so that if they need to come in they can do so. Or, should they end up in one of the local hospitals, then we can catch up with them there as well and try to either get them out of hospital if that’s what we need to do, or make sure they’re being treated appropriately there. I love that breadth of service we can offer.
And of course, you get to work as a team. Working as a multidisciplinary team is probably the most enjoyable part of this type of work. We’ve got excellent colleagues around who we can work alongside, sharing ideas and perspectives, and you can see life from different points of view.
What do I love most about my job? … it’s the multidisciplinary working, being able to work alongside so many skilled colleagues who are enthusiastic and dedicated to what we do. The honour of walking alongside someone in that last year of life, being able to see them in their own home, really feeling like we make a difference, and work holistically.
Justine Robinson
Justine Robinson: I manage the occupational therapy team, the physiotherapy team, and what we call our wellbeing team, which are our wellbeing practitioners who run most of the groups within our Therapy Centres, which is where patients come in for the day and attend groups that are suitable for them.
What do I love most about my job? I’m probably going to echo a lot of what Andrew has already said; it’s the multidisciplinary working, being able to work alongside so many skilled colleagues who are enthusiastic and dedicated to what we do. The honour of walking alongside someone in that last year of life, being able to see them in their own home, really feeling like we make a difference, and work holistically. Often, in England, in the NHS, occupational therapists get separated into mental health or physical; in hospice care, you’re working holistically across all of those areas to get the best possible outcome for the patients, which is something very special.
What are we waiting for? – Hospice care timelines in the UK and North America
Dr. Samantha Winemaker: At what point in a person’s illness journey do you begin to interface with them?
AT: A very good question, and one of much debate in the UK. On average, I think it’s about 40-41 days before people die, if you look at the national work on this. We’re probably slightly better than the average, but around that figure, which isn’t really a lot of time to try and identify all of the troubles and difficulties that have built up over someone’s lifetime, or for their family to get on board, to get people adjusted to where they are and make plans for the future. It’s a very short period of time; however, you will also ask me, “When is the ideal time?”, and that’s always tricky to know as well. The old adage is, “Would you be surprised if this person dies in the next year?”, which is what the Gold Standards Framework started off with. I think this is a good thing to consider.
HS: In the US and in Canada, the average amount of time that people get palliative care is about 18 days before death.A systematic review from a group in Belgium, led by Dr. Luc Deliens, showed 18 days, too, internationally. It is very late.
I wonder if the early palliative care approach needs to be defined by time, when it’s really about the diagnosis and the needs. How do you manage those two pieces – the, “Would you be surprised… ?” question that triggers all these other things, but also realising that maybe people have more complex needs early on in their diagnosis and this awareness that there will be a progression.
AT: Completely; it should be based on needs, not time. There is a time element to it, because people have to recognise they’re coming towards the end of their lives, but it shouldn’t be based on the time. The Royal Marsden Hospital did some work where they screened their palliative outpatients; they found that some with the highest needs still had very good performance status. They weren’t the ones who would traditionally be referred on to palliative care, but when they asked them, their needs were great – and a lot weren’t necessarily physical, but more existential, psychological or social needs.
To me, one of the most important things we do is to get people over this hump, this recognition that they’re dying, so they can still live on the other side.
Dr. Andrew Thorns
There’s also something about the person’s place on that journey. To me, one of the most important things we do is to get people over this hump, this recognition that they’re dying, so they can still live on the other side. For some people, that’s a really difficult mountain to climb, to get over this idea that they’re dying and work out how to adjust to that. For others, it’s very straightforward and simple, but if you can identify those people who struggle early on, perhaps those who are going to have a difficult time at some point in the future, they’re the ones it would be nice to get involved with early, because then we can start to work with them.
JR: Definitely. Pilgrims has tried to address this by offering some wellbeing groups that accept early referrals, so they don’t necessarily have to be a full service user. They can come in and get the information and education they might need about managing breathlessness, or fatigue, or building resilience around their diagnosis and coming to terms with that. They can get what they need, then be discharged back to their primary caregivers in the community. We’re looking at how we can do that, and how patients can weave their journey in and out with the hospice. That might help people feel comfortable with coming to the hospice at an earlier stage.
Walking through those doors takes a lot of bravery. It’s not just about getting practitioners to refer early, it’s about making it a place where people feel comfortable to come early.
Encouraging clear, honest conversations by taking a palliative approach to care
SW: I can appreciate how complicated it is for people to understand what palliative care is, who provides it, how they can access it, when they need it and how they can voice that they don’t want it. People are so confused by the term.
Here in Canada, we’re spending a lot of time trying to separate the idea of palliative care speciality services, and the philosophy of and approach to palliative care. We’re trying to infuse a palliative philosophy alongside any kind of disease management treatments, ebbing and flowing from the time of diagnosis of a non-curable illness, so that philosophy is woven in by all nurses and doctors. So it’s never labelling anyone ‘palliative’ at a point in time, it’s just the natural dance we do across these management styles. A palliative care team or speciality group would come in at intervals from the time of diagnosis until death, when needed. So many people think that palliative care is reserved for the last year or days, or only provided by specialists. What do you guys think about that, this idea that it should be a philosophy or approach to care for any of these illnesses that we know are not curable?
AT:You speak very powerfully about this and I think you’re quite right. Dame Cicely Saunders, when she started all this off in the UK, felt that hospices wouldn’t exist after a period of time – there wouldn’t be a need for them, because you’d just instil that way of working, that approach as you describe it, and therefore you wouldn’t need these other people to do the work for you. It would just be integrated and part of general healthcare. I still really hope that’s something we might do, because good palliative care is just good clinical care. Although there’s still that need for those slightly more complex situations, so I don’t think we’ll completely get rid of the need for the expert side of things.
SW:When I first trained and graduated, I thought I was going to be a pain and symptom specialist doing this most incredible, innovative stuff to improve peoples’ symptoms. But to be honest, 99% of the time, what people are missing is information, and I help them connect the dots – what’s happened to them, where they’re at now, and where they’re going. There is so much more information sharing than dabbling in peoples’ symptoms.
Do you often have people who, by the time you meet them, are really feeling in the dark?
AT and JR: Yes.
The minute someone is full of fear, they shut down listening, they can’t take in any more information. Sometimes, they just need to get stuff out before they can take anything else in. That’s a big part of what we do. We give people space to be able to explore that and come to terms with what’s happened to them, where they are, and be able to really hear, in a more clear language, what is possibly coming next.
Justine Robinson
AT: I agree. In that very famous study by Temel, where they looked at lung cancer patients, a lot of the work they ended up doing was about information, listening and helping people to make decisions. I think we do a lot of that, especially at the hospital. You see people in hospital beds and they’re fearful, frightened, and no one’s taken that time; they’ve been talked at so much, but no one has actually stopped to listen to their concerns, their ideas.
JR: We still see people who, because of the language we use, don’t have an understanding of what’s happening to them. Kathryn Mannix talks beautifully about using “the D words”, but even before that, I’ve met patients who’ve gone, “I’m not sure if I do have cancer, love” because they’ve been told they have a ‘node’ or a ‘nodule’. We really need to be careful of our language at all stages so that patients have a very clear understanding and feel they’ve been listened to. The minute someone is full of fear, they shut down listening, they can’t take in any more information. Sometimes, they just need to get stuff out before they can take anything else in. That’s a big part of what we do. We give people space to be able to explore that and come to terms with what’s happened to them, where they are, and be able to really hear, in a more clear language, what is possibly coming next.
SW: I just came from a home visit this morning. This gentleman has a pancreatic cancer and he is going to start chemotherapy. He has no idea about why he’s having chemotherapy, what the goal of it is. He has very little understanding of what stage his pancreatic cancer is at. I’m smiling and being very kind, trying to be helpful, and in my mind I’m thinking, “That’s not informed consent.” People can argue that maybe he was told but he was overwhelmed so he just forgets. But I’ve been in clinics, and often people are discussing treatment options without helping people understand what the goal of the treatment is, and in the context of where they’re at in their illness journey. I leave every home scratching my head.
JR: One of the most important things we can open with is saying, “Tell me what you understand about your illness.”
I do also wonder if there’s an innate fear of death that we all have. Patients have that so they don’t want to go near there, but if some of the professionals have that too, they’re not prepared to start going down that side of the road. It’s never going to move on from there if neither of us are going to start talking about it.
Dr. Andrew Thorns
AT: If you can get people over that adjustment to the fact they are going to die from this, but they can carry on living (and we can show them how to), that’s achievable.
We have an Advanced Communication Skills course here at the hospice. A couple of times, oncologists have come on and said, “What I’d like to do is, in a 10-minute slot, get someone come in expecting chemotherapy and leave comfortable with the thought that they shouldn’t have chemotherapy.” We go through the techniques, the approaches, the Silverman, Kurtz and Draper model, which a lot of medical schools are using now. Both times, they’ve achieved this; so in 10 minutes, a patient comes in expecting chemotherapy and leaves confident and satisfied that they shouldn’t have chemotherapy, it’s not the right thing for them to do. I think there is a skills issue, and if we could spread those communication skills a bit further, I suspect that would help.
I do also wonder if there’s an innate fear of death that we all have. Patients have that so they don’t want to go near there, but if some of the professionals have that too, they’re not prepared to start going down that side of the road. It’s never going to move on from there if neither of us are going to start talking about it. That dance is going in the wrong direction.
A communication toolkit for healthcare professionals, patients and families
HS:I love the idea of training for advanced communication skills. It’s been happening in different ways in Canada and in other parts of the world with mixed success, I think. Part of The Waiting Room Revolution was to take the ideas behind that clinician training, but make it more public-facing. What do you think about that, the idea that we can coach clinicians to guide people through these conversations – do you think we can also coach patients and families to initiate and walk through these more gentle conversations as well?
AT: That’s a very good point.Absolutely.
Just to go back to my oncology colleagues. They weren’t trying to be dictatorial about this; these were patients they suspected probably wouldn’t (or didn’t) want chemotherapy treatment, so how do they explore that rather than it just becoming a routine? And certainly, the skills we taught them were about getting the patient to talk and seeing where they were.
Your point about developing patient skills, yeah. You see it, don’t you? We come across the patient who has just been suddenly referred to us, it’s a new diagnosis and they don’t know what’s going on or how to deal with these situations. And then you get the other patients who’ve been in the system for some years and they know how it works – they know how to get hold of the consultant secretary, and that they can demand or ask for this or that to happen. They become almost like professionals because they know how to work the system, how to ask the right questions.
I don’t know about you, Justine, but talking to a number of patients who’ve got an appointment coming up, I say, “Well, why don’t you ask these questions? Let’s think about the questions you want to ask. If you ask it this way, or maybe I can send an email and just start that discussion, then when you’re there the consultant is ready, knowing what you want to talk about.”
But I quite agree. I’ve never run a session for patients or relatives about how to manage their side of the consultation, but I love the idea of it.
HS:Justine, do you see that when you’re doing your training? That idea of wellbeing, palliative care must always be just underneath the surface of wellbeing, I would think.
JR: Yes, absolutely. From my own communication point of view, I’ve done the advanced communication skills course, and the most important skill you’re taught on that is to listen, ask a question, and then sit back. What comes out of that is a shorter, more focused session because you’re allowing the person to focus you on what’s important to them.
It’s a really bold idea; I like it, the idea of us perhaps training families and patients in how to do that. I think we probably do, on an individual level. When we’re talking to people as a therapist or in the Therapy Centres, we will often have those conversations and say, “Have you thought about this?”, “Maybe if you ask…” or “Have you thought of suggesting… ?” Sometimes it’s about the patient knowing that they’re at the point of wanting to stop treatment, they don’t want the chemo or the radiotherapy anymore. Often it’s about helping to manage those conversations with their families and their medical teams, and saying, “Have you thought about discussing it like this?”
So yeah, I think we probably do that one-to-one quite often.
Empowering patients and the public to advocate for themselves
SW: This is how we ended up doing the podcast series. We were doing all these one-to-one-type interventions, arming people with the types of questions that they could go to the healthcare system with and perhaps leach out more information than they had before they asked the questions. But they don’t all get to see a palliative care specialist in their home. We know we only really see the tip of the iceberg of the people who could benefit from our skills.
We got really frustrated with how slowly things were going training healthcare providers as the middle people, so that patients and families were able to get the information they need. We decided: we’re going rogue. We are going to be public-facing. We are going to share this one on one stuff we’re doing, the types of conversations we’re all very comfortable with, but we’re going to deliver it right to the people so that they never, ever have to worry about someone identifying them as needing palliative care. So that naturally, if they do this well, they will automatically get it from the healthcare system just by being a different kind of patient and family – more activated, more empowered, more armed with the right stuff.
JR:I think there’s something to recognise there about privilege as well. In east Kent, we serve very different socioeconomic groups. When I’ve had to navigate the system on behalf of someone very close to me – one, I have a healthcare background, but also I’m white and educated and fairly confident about speaking my mind. But we also see lots of families who aren’t. I don’t know if you have the term ‘white coat syndrome’? When they see a doctor, they become very passive because they feel, “Well I don’t have an education. This is the person who knows everything.” It’s those people I’m really interested in how we empower as well, and how we make sure their voices are heard in the system, because we know with healthcare outcomes that they’re the people who perhaps aren’t getting the same service.
We decided: we’re going rogue. We are going to be public-facing. We are going to share this one on one stuff we’re doing, the types of conversations we’re all very comfortable with, but we’re going to deliver it right to the people so that they never, ever have to worry about someone identifying them as needing palliative care. So that naturally, if they do this well, they will automatically get it from the healthcare system just by being a different kind of patient and family – more activated, more empowered
Dr. Samantha Winemaker
SW: It’s so true what you say. In our city, we have a mixture of socioeconomic statuses. But I will say that I assumed that people who had higher education, more money, would maybe fare better when facing a progressive, life-limiting illness, but it hasn’t always been my experience. There are other ingredients that seem to bubble to the top, that almost predict whether or not people are going to fare well or not.
I appreciate totally what you’re saying, Justine, but I do find that the darnedest people have someone in their life who’s that go-getter, the organiser or the manager. They’re like a dog with a bone, they’re just that kind of assertive person. When I find people like that in the person’s environment, I think, “Oh, OK, this is going to go better than a bunch of people who are just going to let the healthcare system blow them wherever they go.” Someone who’s assertive makes a huge difference, or just someone who naturally has that style, a curiosity or they ask a lot of questions, they won’t stop until they understand something. Even if their education level is lower, there’s something about different personalities that fare better than others as well.
We meet so many different people, don’t we? I don’t think it’s a one size fits all, that’s for sure. I think what you’re saying is, we have to appreciate that there is such diversity, and empowering people is going to look different depending on who you’re trying to activate.
HS: I know some people don’t like the word ‘empower’, but every person should have an understanding of what their illness is, where they are in their illness, what might the future look like, what the intent of the treatment is, what the options are. I would imagine medical professionals are trying to answer those questions, but these are very important cornerstones of what is happening, and if people get lost in that, they lose their control and the ability to make choices that are good for them. That’s irrespective of finances etc.
Encouraging curiosity to create bespoke care
SW:Just a point of clarification. When we talk about moving these types of conversations upstream, it’s not really about talking about death and dying when someone’s first diagnosed with an illness that might have a life expectancy of 10 or 15 years, like dementia. Or five years, like amyotrophic lateral sclerosis (ALS). It’s not sitting people down and saying, “Look, you have to know, this is going to end in death.”
I just wanted to clarify that. It’s really about us sharing, with patients and families, that every one of these illnesses is uniquely felt by the person, but it is not the first time we’ve seen this illness. People have a right to know that this illness has a pattern to it, right from the get-go, if they want it; that is has these milestones, these bus stops, these major decision points along the way.
… the people that ask more questions feel more grounded and more prepared. Infusing an early palliative approach is not about talking about death and dying (unless the person wants to) right from diagnosis – it’s about helping them know that there is a roadmap.
Dr. Samantha Winemaker
I welcome you to ask us more about that, because the people that ask more questions feel more grounded and more prepared. Infusing an early palliative approach is not about talking about death and dying (unless the person wants to) right from diagnosis – it’s about helping them know that there is a roadmap.
AT: One of the keys is about customising your order, as you put it. Tailoring your care plan to your preferences. I think that’s the thing, isn’t it? Some people like to know every single bit of detail right there and then – “Plan the rest of my life for me.” For other people, it’s a much more gentle journey, step by step. Or maybe not wanting to know at all. So it’s customising, as you put it so beautifully, to that person’s needs.
JR: And introducing the idea of advance care planning at that early stage, and it not being necessarily about just a death plan. But actually, being able to prepare for those changes in advance, knowing the broad strokes of what your illness is possibly going to do for you, and having those plans in place. So the next step might be you’re not going to be able to do your stairs at home, so what are the plans going to be? Would you like to get those in place now so that we’re not hitting crisis?
AT: Sammy, if I was to disagree with you slightly – although everyone experiences individually, there are certain patterns that emerge, aren’t there? There are certain things that tend to happen to certain groups of people in certain ways. So we have that knowledge, and somehow we have to use that just to start to plan ahead. I think that’s important.
But quite right, it’s not just about the medical need, although sometimes that seems to take a prominence in those situations.
SW:It’s very rare when I ask someone if they’re interested in more information about their situation that they say, “No, we’re not interested.” In fact, rarely has someone said no. Sometimes they get a little bit sheepish and worry what I’m going to say, like tell them that they’re going to burst into flames at the end. They have all these ideas that they’re worried you’re going to confirm for them. But aside from that I’ve rarely, rarely, rarely ever met someone who has said, “No, we don’t want to know.” If they do say it, usually it’s because they’re scared of something; then you unpack that a little bit, then they realise there’s some course correcting we can do to make them feel better.
JR:I know I’ve been guilty of this in the past, particularly when I started in palliative care, with going too fast. We’re maybe taking them five steps down the road, and actually this person can only do the first two, or one, or even half a step. It’s about working with that person and walking alongside them at the pace they can do that.
SW:I love that. So not just inviting people, but actually assessing or asking them the degree to which they want information, and how they want it.
The importance of effective communication and the future of end-of-life care
AT:Sammy, do you think that’s something to do with you in your communication skills, though? Do you think people choose the people they want to ask these questions to? If you’ve got someone who you get on with, you have a bond or a trusting relationship with, you feel safe with, then they’re the person with whom you’re going to think, “Yeah, I want to explore this.”
Whereas to somebody else, you perhaps don’t quite hit it off, or you’re not quite confident about them, then you’re less likely to go into those more sensitive areas.
SW:I think so, for sure. I think that because I’m in their home, they probably feel even more comfortable – aside from who I am, just being in their own environment, they can be themselves. So definitely, I think the right person at the right time at the right place makes a lot of sense for these conversations.
I’ve had medical students and nurses say, “You just took an hour to do all of this. How can you expect other people, in their busy clinics, to take so much time?” Time is everyone’s concern.
What I usually say to people is that the reason why it’s taking me an hour is because I’m meeting this person at this stage of their illness. I’ve never met them before. There’s been lots and lots of doctors and nurses involved, who have perhaps been busy doing other things or uncomfortable having these conversations, so it’s requiring an hour of my time right now.
I’d like to think, if we do this well, in 20 years let’s say, that people will have bits and pieces of this conversation along the entire journey so that no one person is responsible for the one-hour discussion at the end. There will always be the one-hour discussions, but you know what I mean; it shouldn’t be the first time they’re invited into an honest, open discussion about their illness when they meet me in their home when they have, on average, a couple of months to live.
AT: Yes, I quite agree. It takes me back to Dame Cicely Saunders and her idea that we would do ourselves out of business, which maybe we still might. Your work on the podcast, the communication skills stuff, maybe that might just change that culture in due course, by the time we retire.
SW: I think there’ll always be a role for us. Kathryn Mannix set me straight, too, because I was trying to convince her that we shouldn’t exist. I think there’s always going to be a role for us for complex situations, complex discussions. But I would say that 99% of what I do could be done by any well-intended and well-skilled doctor or nurse. There are some complex things we do, but for the most part, I think that it wouldn’t be a far stretch to teach all OTs, physiotherapists, nurses, doctors, social workers, to learn a palliative approach.
What’s next for Pilgrims Hospices?
HS: It would be remiss if I didn’t talk a little bit about some of the fundraising challenges that exist – in Canada, but I would suspect in the UK as well. I think I read somewhere that the National Health Service (NHS) covers 20% of Pilgrims Hospices’ budget, so 80% of your operating budget, which is almost £11 million in a year, is fundraised each year by local residents? On some level, that’s a testament to the impact you have on the community because they’re so behind you year after year. But it must be a challenge. How do you think about that as you’re programming and planning ahead and trying to get staff and do all your services?
AT: There’s 750,000 people who live in east Kent and they raise the £11 million every year, so we are hugely indebted to them. You’re quite right, it demonstrates the importance people place on this type of care, which is great. It does raise that question, where does the hospice charity fit? We are a community provider, how do we influence the community around us?
We were talking earlier about when should people start talking or thinking about these issues, sohow much do we start bringing that work into the community? How much is it about us providing or doing to the community? How much is it about us enabling the community to do it themselves, to take on that responsibility themselves? There are huge discussions and debates about that, quite rightly, because hospices originally were a protest movement; they originated because good care wasn’t there for people, and it was an alternative.
We’re absolutely indebted to the people of east Kent, they’re just outstanding in their creativity, how they raise money for us each year. I remember being told once that around 1 in 7 people know someone who’s been directly cared for by Pilgrims Hospices in east Kent, so that’s the kind of personal feeling that the people of east Kent have about our services and what we do.
Justine Robinson
So what are we doing as a social movement now? How are we trying to engage with our community?
We’re starting up a THINK project. We’re just starting to identify people who are perhaps early-ish on in their journey, just getting them to start thinking about it – not about death and dying, but just to start thinking about the future. What is important to them? What do they need to do? What do they need to think about going forward? Are they engaged with their families about what’s happening? What do we need to put in place? It maybe just starts that journey, starts that discussion.
It’s one way that we can start to empower the community; and perhaps not just those people who are poorly, but taking that out to businesses, to corporate organisations, and get them thinking about it as well. Because as we know, talking about dying doesn’t make it happen, but if you haven’t had that conversation, haven’t started engaging in that process and that journey, then of course it ends up being very difficult at certain times.
I suppose an advantage to us being a charity is that we can then do the things that we think are important. We’re not under government control to meet targets or to do things in a certain way. So we quite like a certain amount of flexibility, but a little bit more cash from our health service would be very helpful. What do you think, Justine?
JR:Yes, I agree. We’re absolutely indebted to the people of east Kent, they’re just outstanding in their creativity, how they raise money for us each year. I remember being told once that around 1 in 7 people know someone who’s been directly cared for by Pilgrims Hospices in east Kent, so that’s the kind of personal feeling that the people of east Kent have about our services and what we do.
With THINK, we’re piloting it in 2022. To start with it will be staff running the THINK sessions, but the hope is that it will become expert volunteers. So eventually, it will be the community running these sessions for the community; we will offer the training. It’s that idea of advance care planning at an earlier stage, it not necessarily being about just your death plan, but actually all the other things you can think about along the way as part of your advance care plan. That’s why we’ve called it THINK; we just want to drop those seeds in and hopefully something will take root and we’ll just help people start having those conversations.
… as we know, talking about dying doesn’t make it happen, but if you haven’t had that conversation, haven’t started engaging in that process and that journey, then of course it ends up being very difficult at certain times.
Dr. Andrew Thorns
SW: That’s amazing. How can we support your work? Donate, right?
JR: Yeah! Obviously, you know, sharing everything we do when you see us on social media, supporting us that way is always really helpful too. We’re very lucky in the way that people donate and get involved. And volunteer – volunteers are the lifeblood of the hospice, we wouldn’t be able to run without them. Certainly, over COVID when we couldn’t have volunteers in the building because we needed to stop footfall, we really felt the lack of them because they’re such a joy to have around.
AT: And collaborate I’d throw into that as well, Sammy. You’ve got some great ideas from what you’ve developed here, we’ve got good ideas. The fact that we can come together internationally and share those good ideas, that all helps. If the service can get better, that really helps. So if we evaluate the THINK project and it works and it changes the way people approach things, and we share that with other people, then that’s good.
HS: Justine and Andrew, I really want to thank you both for joining us today and being on our podcast. It was such a pleasure to connect and I hope that we can continue to collaborate and contribute to your amazing work.
SW:We can’t wait to learn from you guys. It seems like you’re always at least ten steps ahead of us, so do share.
AT: I’m sure you’ll catch us up very quickly, Sammy, if that’s the case. It’s been an absolute pleasure.
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.
7th December 2022
A Colourful Death
Photograph: Saijal Reahal with her mother, Bina
Saijal Reahal talks us through her struggle to come to terms with having a chronically ill mother and her visualisations and notions about death, versus those of people around her.
I was nine years old on my school sports day when I discovered my mum had an incurable autoimmune disease that she had kept from me since I was born. I only found out because I was crying that she was the only mum in my friendship group who did not volunteer to participate in the parents’ sack race (horrific, I know). She wiped my tears and said, “I’ll tell you later”.
At home, I learnt that it was lupus, and not lack of love, that made her think twice before throwing her delicate bones around.
I was heartbroken. I couldn’t fathom that an illness had rattled her bones, joints and several organs, that she felt fatigued most days, that it wasn’t safe for her to deliver a baby, and that in spite of all of this, she had barely told a soul, including me.
The day after, I envisioned her funeral. I fired out questions that were only permissible to be asked by a child: “Are you going to die?” “Will I get it and also die?” “How will Papa cope without you?” His cooking skills were, after all, only average at the time.
We created an environment where it was safe to speak about death, with hope, lightness and even humour.
Saijal Reahal
Over the years, I was repeatedly reassured. Whilst some days were tough for me, as an only child, and Papa, the strong medications meant Mum could enjoy a good quality of life, her attitude made her consider it a great quality of life… and Papa got better at cooking. We created an environment where it was safe to speak about death, with hope, lightness and even humour. I asked Mum how she would want her send-off to be to the level of detail of: casket open or closed, commiseration or celebration, and which one of her lipsticks I would wear.
The day she passed away at 61, 17 years after that sports day, was still unexpected. She complained of a more intense type of pain in the morning, and within a few hours she was gone. Given the way her illness had worked in the past, with good periods and bad periods, we thought we would get a bit more notice. But, I did feel like I had braced myself for losing her from all of our conversations, post-sack race. I focused my efforts on organising the funeral to do her justice. I would stick to our traditions as British Indian Sikhs, whilst making it colourful, majestic and different, to match her vibrant character.
However, support was not easy to garner from all family and friends. Some were sceptical about doing things in such an upbeat manner. They were not comfortable with the idea of wearing colour or bright lipstick as some of my cousins and I had planned to do in honour of Mum’s style. Having the casket closed also sparked some controversy; I got advised it may be seen as “exclusionary”. And I was told I was probably in shock or denial, especially as I had not cried after the initial 10-minute shock. I came to learn that I was not grieving the traditional way.
I believe talking about life, death and all the ugly bits in between, made coping with both a chronically ill family member and bereavement, easier.
Saijal Reahal
Across much of Indian culture, when someone dies, people will arrive almost immediately at the home to pay their respects. And when I say people, I mean everyone the deceased may have ever spoken to, even if they have not seen them in decades. Here, they will pray, talk and eat. This can go on for close to 24 hours a day until the funeral. Luckily, my aunties pretty much moved in and were resident chefs and chaiwalas, catering for the masses of guests and keeping everything spotless. The support of the community was beautiful and a testament to Mum’s people-adoring persona, but nobody prepares you for the gaping hole it leaves when everyone packs up and goes the day after the funeral.
It is also the norm for people to visibly exhibit that they are mourning – that equals showing face at the house, not wearing colour, weeping and even wailing. I found this hard to come to terms with, particularly with those who who were not close to Mum. The Sikh religion does not advocate the need for public, ritualised displays of mourning and, actually, encourages releasing yourself from your interpersonal attachments and letting the deceased go with dignity and good blessings for wherever their soul travels to next. Yet, it seems to be hard for people to break centuries-old “traditions”.
Saijal on the day of her mum’s funeral
Over the course of the funeral planning to the day itself (which was exactly as splendid as I had wished for Mum), people became more relaxed and open-minded, myself included; after all, there is no right way to grieve. I think their initial discomfort stemmed from death still being a taboo in our culture, and wider society, until it happens – then everyone wants to know and be involved. I was able to talk about death and what happens next relatively freely in my household, but it can be considered morbid, inappropriate, improper.
I also reflected inwards. Perhaps my lack of tears was not so noble. I tried to show I was doing OK. I could not stand people vocalising their pity for losing my mother suddenly, especially at a younger age, when I was navigating my troublesome twenties and did not have a family of my own. My pride was reflective of Mum’s. She fought lupus for over 40 years but kept it a secret that she shared with very few people. I often encouraged her to blog about her experience from the lens of a South Asian sufferer, particularly as she had a science background and a PhD, but she refused. Neither of us, in times of physical or mental pain, wanted to appear weak and risk being gossiped about in the community. Being this vulnerable now is certainly daunting.
But, I believe talking about life, death and all the ugly bits in between, made coping with both a chronically ill family member and bereavement, easier. I have fond memories of Mum and I nattering away about her “loopy lupus”, the bruises she would get after blood tests and injections (“What’s this a map of, Mum?”) and that infamous sack race that changed the course of our mother-daughter dialogue forever.
Mum taught me that death is not the opposite of life; it is the consequence of life – of having breathed, experienced, felt and loved.
You can find more about Saijal’s story in Letters from the Grief Club, an anthology of short works from people who have been bereaved.
Saijal Reahal
Saijal Reahal is a part-time Financial Services consultant and a full-time mental health advocate who has publicly spoken and written about her experiences with depression, trauma and grieving, and how she uses fashion and performance to heal herself. In 2019, Saijal lost her mother to complications of systemic lupus erythematosus, an autoimmune disease she had been suffering from for over 40 years. Through her writing, Saijal seeks to destigmatise and put some colour around chronic illness and death.
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.
29th November 2022
This Grief Thing: Helping people to talk about grief
Photograph: This Grief Thing Middlesbrough 2018 by Fevered Sleep
Following the devastating and sudden death of his sister, David Harradine, Co-Artistic Director and CEO of arts production company Fevered Sleep, launched This Grief Thing.
We live in a time when many people find grief impossible to talk about. David explains how This Grief Thing aims to normalise conversations about grief, helping people to support each other through a universal human experience.
It’s 24 November 2011, the night my life changed. 6:50pm, and I’m in my studio in London, editing a short film about ageing and time. My phone rings. My sister-in-law’s voice, “David… I don’t know how to tell you…”. In the background, my mum, wailing, screaming, pain. A sound I will never, ever forget. “David… I don’t know how to tell you…”
On 24 November 2011, my life changed. My older sister, my closest sibling, had died in a car accident. Immobilised with shock, I called my partner. He came to collect me. We drove back to our flat. In the kitchen, I smashed things up. We got in the car, we drove up the A1 to my parent’s house in Yorkshire, the house where I grew up, and I stayed there for the next three months, in a house of grief, in shock, in my childhood bed, trying to help my parents, trying to come to terms with what had happened.
Again and again, we heard about invisible grief, unacknowledged grief, grief that had to be hidden, silenced, ignored. We talked about mourning clothes, about wearing black, or arm bands, about the different rituals in different cultures and religions and countries, all the different ways that grief could be worn on the surface of the body: “I’m still grieving: talk to me about it.”
David Harradine
During that time, I felt completely disconnected from my former life. I stopped working, focused completely on my parents and all the ways I might be able to help them survive this loss. Cooking for them, eating together, crying together, visiting my sister’s grave. I tried to fill the abyss that she had left behind; trying to take up the space of two children; trying to produce that much love.
For myself, I felt as though a veil had lifted, a veil that had been obscuring a whole emotional landscape that I didn’t know existed. A landscape of loss, and death, and grief; a landscape I was completely lost in, confused and angry and heartbroken; a landscape for which I had no map.
This Grief Thing Preston 2018 by Garry Cook
I am lucky. I work in the arts. I’m co-artistic director of an arts production company called Fevered Sleep. My friends and colleagues are in tune with their emotions, sensitive and articulate, and they were amazing; an amazing support, unafraid of my grief, it seemed; able and willing to acknowledge it. My mum had a very different experience: seeing people turn away when they saw her in the supermarket; going out for coffee with friends who didn’t ask her how she was. As though being a grieving mother was a disease, something contagious, something to avoid. Or something just too awful to acknowledge. But one by one by one, my friends also stopped asking how I was, how my parents were; stopped asking about my sister. After a few months, everybody else seemed to be back to business as usual. Me? I was still in the thick of grief, still in shock, still bewildered, and increasingly angry and disappointed that those people who had been so amazing at the start had one by one by one forgotten to ask how I was; had forgotten how to see and acknowledge my grief.
One day I said to Sam Butler, Fevered Sleep’s other artistic director and my best friend, “I want to make a T-shirt that says: ‘I’M STILL GRIEVING: WHY HAVE YOU STOPPED TALKING TO ME ABOUT IT?’”. Without hesitation, Sam said, “Let’s do that, let’s make that happen, let’s make that for you”. And so our project This Grief Thing was born.
This Grief Thing Preston 2018 by Garry Cook
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing Manchester 2019 by Richard Tymon
This Grief Thing London 2021 photo by Method Films
This Grief Thing London 2020 by Paul Akinrinlola
This Grief Thing London 2021 by Method Films
This Grief Thing London 2021 by Method Films
This Grief Thing London 2021 by Method Films
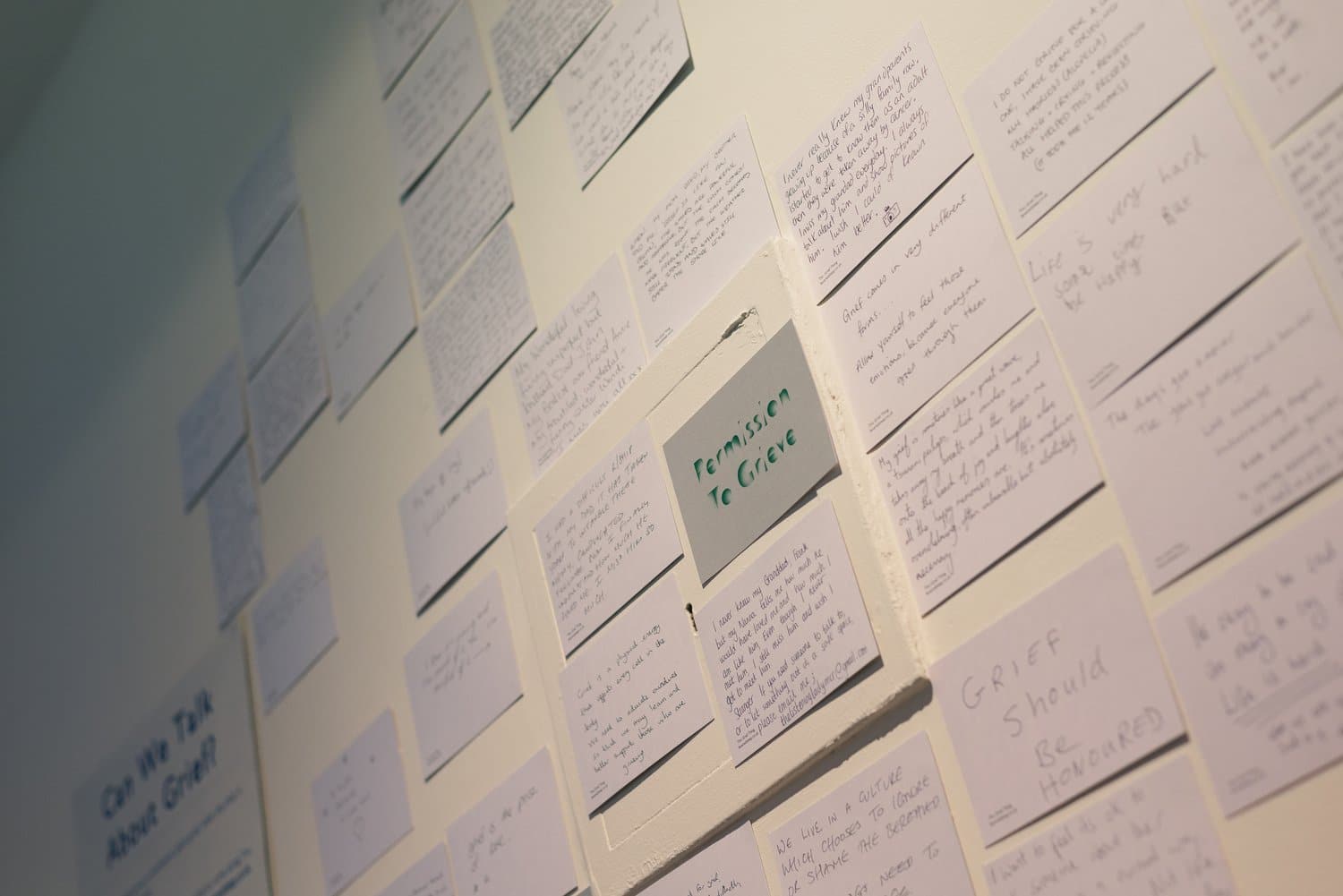
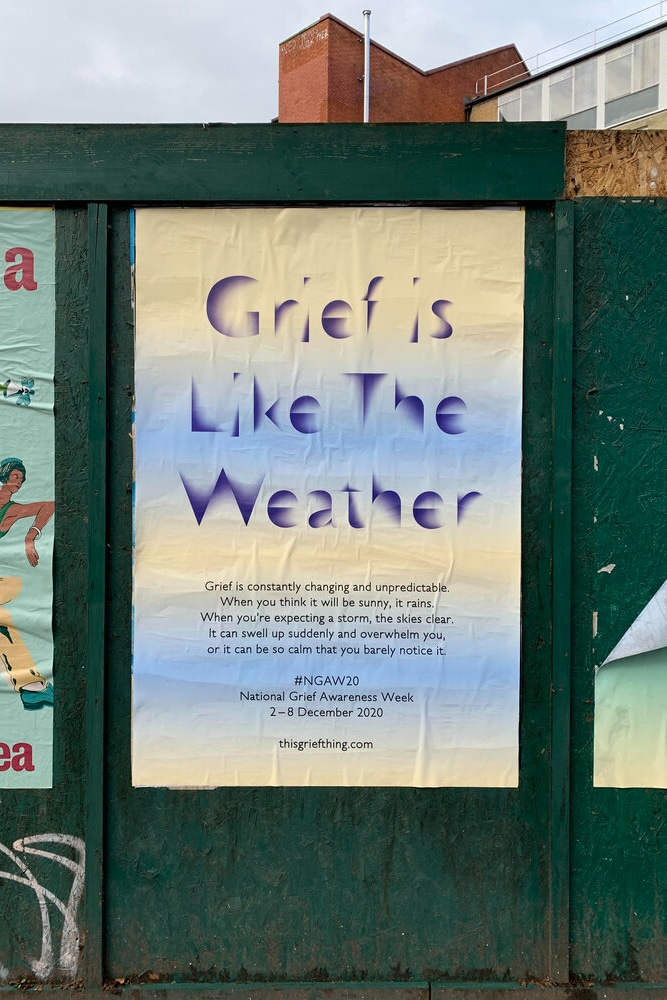
We began as we always do when we’re making a new project: by talking with other people about the thing we are working on. Over several months, we travelled the country, meeting small groups of people to talk about grief. We gathered stories, advice, words and phrases that we heard repeatedly. Words that attempted to describe grief; words that might be useful for someone who’s grieving: Grief is like the weather. Grief = Love. Don’t panic if I cry. Let me be sad. There will be joy again.
This Grief Thing London 2020 by Fraser Muggeridge Studio
Again and again, we heard about invisible grief, unacknowledged grief, grief that had to be hidden, silenced, ignored. We talked about mourning clothes, about wearing black, or arm bands, about the different rituals in different cultures and religions and countries, all the different ways that grief could be worn on the surface of the body: “I’m still grieving: talk to me about it.”
Sam and I worked with a graphic designer, Fraser Muggeridge studio, and made a collection of clothing – T-shirts, jumpers, scarves – as well as things like cards and brooches and badges. Every item showed one of the phrases that we’d gathered through those conversations about grief: Let me be sad; Grief = Love; Don’t panic if I cry
Once we’d made this collection, we travelled around England, opening pop-up shops. The shops became places for people to gather to talk about grief. We sold the items on a pay-what-you-want basis (someone might pay 50p for a jumper, someone else £50). Hundreds and hundreds of people came to talk, to listen, and to learn about grief. When the shops were closed, we held more conversations, which we called Grief Gatherings. These became a vital, central part of the project, and when the pandemic arrived in 2020, and meeting in person was no longer possible, we moved the Grief Gatherings online. Suddenly we found ourselves in conversations with people all over the world: people in the UK talking with people in Canada and Australia, France and Belgium and the USA. As the project grew, we invited other people to host conversations for us. Brilliant guest hosts engaged people from their own communities. Deaf actress and producer, Deepa Shastri, held Grief Gatherings in BSL; queer activist Dan de la Motteheld gatherings for LGBTQ people; multidisciplinary artist Lou Robbin held them for people from the Global Majority.
This Grief Thing has tried to make grief more visible. It’s an attempt to normalise grief, to insist that it’s a normal, healthy emotion that shouldn’t be hidden or suppressed; that grief isn’t something to be ashamed of.
David Harradine
In 2021, we put together a whole programme of events in London: we opened market stalls instead of shops; we ran a billboard and poster campaign, trying to make grief visible in public spaces; we did many more Grief Gatherings; we commissioned artists Akshay Sharmaand Rayvenn d’Clark to make work on the theme of grief. We also curated a series of online conversations on grief, which brought together various ‘grief experts’ to talk about grief from their own perspectives. An artist with a philosopher; a death doula with an academic; a photographer with a bereavement counsellor; a theatre-maker with a fashion historian. If you’re interested, you can find recordings of these conversations on our website.
In all these different ways, This Grief Thing has tried to make grief more visible. It’s an attempt to normalise grief, to insist that it’s a normal, healthy emotion that shouldn’t be hidden or suppressed; that grief isn’t something to be ashamed of. Through all the many conversations we’ve had with people about grief, in the shops, in Grief Gatherings, on the street and online, we’ve learned so much, and the project carries this learning from place to place. This Grief Thing is a resource, a community, a declaration, and an attempt to bring grief into the light. Thanks for reading this blog: your engagement is another small step towards acceptance of grief; another small act of radical compassion; another gesture of solidarity in the face of unbearable loss.
As I write, we’re taking a pause from This Grief Thing while we work on new projects. We’ll be doing more Grief Gatherings and another online programme in summer 2023, and all the items from the collection are available from our online shop. If you want to keep in touch, sign up to our mailing list and you’ll be the first to know when the project is running. We’d love to see you at one of our events; we all need to talk about grief.
David Harradine
David Harradine is an artist, and co-founder of Fevered Sleep, making performances, installations, films, books and digital art. He’s Professor of Interdisciplinary Practice at The Royal Central School of Speech and Drama, University of London and is a trustee of Yorkshire Dance. Born into a rural, working class community in West Yorkshire, he now lives in York and London.
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.
8th November 2022
What is an eco funeral?
Eco, natural, or modern funerals, are terms often used to describe a funeral that tries to be more environmentally-friendly. Most of these options aren’t new, but they are becoming more widely available and increasingly popular.
Elle Hogben from Willow and Green Funerals explains just some of the ways that funerals can have a lighter impact on the planet.
People choose eco funeral options for many different reasons.
Some want to lessen their impact on the environment as they die. Others like the idea of being naturally returned to the earth, and enjoy a simpler way of doing things. And some people just like the aesthetic that comes alongside a more natural method; perhaps they love being outdoors or in their garden.
Natural burial grounds
In 1993, Ken West formulated the first woodland burial grounds – areas of cemeteries with no headstones that would have trees planted and be left wild. The popularity of natural burial grounds has grown significantly since then, and continues to do so. There are now over 220 recorded natural burial grounds in the UK. Some council-run cemeteries have designated an area for natural or woodland burials. There are also natural burial grounds on privately owned areas of land, and they can be beautiful, peaceful places to visit.
Their goal is often to create and preserve a natural habitat for wildlife, and try to avoid any non-biodegradable elements, so that everything is naturally returned to the earth. Each burial ground differs on what they allow, and your funeral director or the burial grounds staff will be able to guide you.
The coffins used are usually made with completely biodegradable components, and the same goes for flowers, including no plastic or oasis (also called flower foam), which is a non-biodegradable plastic. Traditional gravestones are not permitted, but most cemeteries allow smaller wooden markers or something similar. Often, a tree or plant of some variation is planted next to or around the grave. The woodland and natural landscape make beautiful surroundings for a funeral service, or for the scattering of ashes.
What does an eco coffin look like?
Natural coffins include materials like willow, bamboo, or seagrass, and are really beautiful. These coffins are completely biodegradable, including their fixings, linings and handles. The lattice method of weaving the coffins also provides a great opportunity for adding flowers. There are even some coffins that are grown and made in the UK, reducing the carbon footprint, including some particularly lovely willow farms in Somerset.
Cardboard is one of the most efficient and cheapest eco coffin materials. For me, a personal favourite is when families choose to have white or neutral cardboard coffins, allowing family, friends and children to draw and write messages on the coffin. Or, how about a coffin with pictures of cats for a cat lover? These coffins provide a great opportunity to personalise a funeral, and get the whole family involved in a precious moment.
One of the most simple options is a shroud. Shrouds are usually made from natural materials such as cotton, linen, silk and many more. Families can then lay flowers and decorate the shroud in the same way they would a coffin. These are such personal choices, which is why it’s a good idea to think about what you might want, to make these hard decisions a little easier for your family.
Funeral flowers have always been a large part of the traditional funeral, from flowers accompanying the hearse, to flowers gifted by mourners. People often ask for donations to charities instead of gifted flowers, or sometimes a mixture of both.
Whilst flowers themselves are biodegradable, oasis is a common element of flower displays, and therefore many traditional displays are not biodegradable. The RHS flower show banned oasis from their displays in 2021 because of its harmful impact on the environment. Fortunately, there are alternatives, such as moss. The majority of florists now provide at least some eco-friendly options. Unfortunately, we only grow certain flowers in the UK at various times of the year, so understandably flowers often have to be imported from across the globe. Chat to a florist or your funeral directors about what flowers they can source more locally at specific times of the year.
Local flower farms are wonderful places to visit; some even allow families to come and browse and choose flowers to be made into tributes. A local florist told me that families sometimes request for bulbs to be added to the floral displays. The family can then take these home and plant them in their gardens – what a beautiful way to reuse funeral flower displays and remember a loved one. A lady once showed me a wonderful display of dried flowers she had made for her mum. I was surprised at how much colour and vibrancy the flowers still had. When dried, flowers can be taken home and shared with the family and enjoyed for a lot longer. It’s great to see that the options available to families are growing.
There are also creative alternatives to flowers.
For example, for a football fan, how about a football shirt on the coffin? I recently saw a Star Wars fan’s funeral had pallbearers dressed as stormtroopers and a Lego Star Destroyer on the coffin (although Lego is made from plastic, the figure may have belonged to the family and have been kept by them afterwards; it would have been removed before burial and therefore wouldn’t impact on the natural environment); how creative!
There are some wonderful craftspeople out there who make beautiful things, like paper flowers made from recycled books that the family can keep forever.
There is no right or wrong answer, and families often come up with some beautifully unique ideas.
Customising a funeral: Orders of service, ashes and more
Orders of service can be made on recycled paper. A wedding I attended used beautiful seed paper for the wedding order of service; the paper is usually made from recycled materials and embedded with herb, vegetable or flower seeds to be planted. This is a lovely idea that reduces waste and can be adopted for funerals, giving guests something special to take home and remember their loved one by. And remember, just because orders of service are a traditional part of a funeral, doesn’t mean they are essential. You might decide to have a single order of service placed for all to see, or send out an electronic version.
A biodegradable urn
There are many beautiful options when it comes to deciding what to do with loved ones’ ashes. Some people like to plant the ashes in urns, and maybe even grow a tree near them. Arboform urns are a great option that will start to naturally biodegrade. However, they can also be used as a display urn, because they will only start to biodegrade when planted in the ground. This eco option comes in a wide range of shapes and beautiful styles; they are often cheaper than some metal, ceramic and wooden urns.
It’s exciting to see the increased use of electric hearses in the funeral industry. But what about all the guests attending? A simple idea such as carpooling is a great way to reduce funeral guests’ carbon footprint. Often, this allows families to spend more time together, and it’s a way of respecting and honouring the wishes of the person who has died, if their preference was for an eco funeral.
These are just a few of the many ways that a funeral can be more eco-friendly. The most important part of arranging any funeral is empowering the family to have choices. As a funeral arranger, it is our job at Willow and Green Funerals to source a wide range of options for families to achieve whatever they want. Traditional funerals still play a big, important part in the funeral industry. All we hope is to show people that they don’t have to sacrifice this in order to be more environmentally conscious.
Elle Hogben
Elle Hogben is a funeral arranger working for Willow and Green Funerals, an independent funeral home in Ashford, Kent. Willow and Green believe in providing personal, high-quality funerals that don’t cost the earth. Elle feels it is a privilege to be able to help people through one of the hardest times of their lives.
Elle has been attending Pilgrims Hospices events for many years with her mum, Annie. She is always impressed by the amazing and vital work that the staff at the hospice do.
There’s much more to death than we think; what if it isn’t just an ending, but an event we can plan for? Thinking beyond the four walls of hospices and hospitals, we have the chance to approach it with confidence and plan a good death. After Wards is a collection of insights and ideas from people who can help us all to re-imagine this essential part of life, and to live well until we die.